Orthodontic & TMJ Treatment
With a Holistic Approach
For your perfect smile, and improved overall health, choose JM Dierkes Orthodontics and TMJ.
Improve Your Overall Health
Become Pain Free
Achieve Long Lasting Results
Welcome to JM Dierkes Orthodontics & TMJ
A Naturopathic Approach to Orthodontics & TMJ

Located in Roswell and serving Sandy Springs, East Cobb, Marietta and the greater Atlanta area, JM Dierkes Orthodontics and TMJ offers TMJ treatment, comprehensive orthodontics, conventional braces as well as clear aligners, myobrace, 2 Phase orthodontic treatment, facial esthetics, nutritional counseling, & sleep apnea appliances. By incorporating naturopathic practices with his medical knowledge, Dr. Dierkes treats the patient as a whole, aiming not only to correct the orthodontic or esthetic concerns, but also to produce the best possible treatment outcomes, establishing lasting results.
Dr. Dierkes has been developing beautiful smiles for his patients for over 30 years. Recognized by the American Association of Orthodontists as one of the top 10 orthodontists in the country, he specializes in early orthodontic treatment, holistic and comprehensive treatment, nutritional counseling, and treatment of TMJ dysfunctions. Educated & degreed in Naturopathic medicine, his goal is to assist patients in arriving at a pain-free status without drugs.
Welcome to JM Dierkes Orthodontics & TMJ
A Naturopathic Approach to Orthodontics & TMJ
Located in Roswell and serving Sandy Springs, East Cobb, Marietta and the greater Atlanta area, JM Dierkes Orthodontics and TMJ offers TMJ treatment, comprehensive orthodontics, conventional braces as well as clear aligners, myobrace, 2 Phase orthodontic treatment, facial esthetics, nutritional counseling, & sleep apnea appliances. By incorporating naturopathic practices with his medical knowledge, Dr. Dierkes treats the patient as a whole, aiming not only to correct the orthodontic or esthetic concerns, but also to produce the best possible treatment outcomes, establishing lasting results.
Dr. Dierkes has been developing beautiful smiles for his patients for over 30 years. Recognized by the American Association of Orthodontists as one of the top 10 orthodontists in the country, he specializes in early orthodontic treatment, holistic and comprehensive treatment, nutritional counseling, and treatment of TMJ dysfunctions. Educated & degreed in Naturopathic medicine, his goal is to assist patients in arriving at a pain-free status without drugs.




Dr. Dierkes has developed an “All Things Considered”
approach to orthodontic and TMJ care

“All Things Considered” considers the relationship of teeth, bone, muscles, TMJ, airway (breathing patterns), food allergies, nutritional deficiencies and excesses, and endocrine imbalances that may adversely influence bone and soft tissue metabolism.
Dr. Dierkes’ own research at the University of Michigan pointed out the importance of adequate amounts of vitamin C for the best connective tissue matrix as a means of providing the most optimal long-term stability. His MRI research pointed out the relationship between a bad bite and damaged jaw joints.
To neglect one area without considering the “whole” will just create imbalances in other areas that will ultimately interrupt the innate need for the body to maintain balance.








All Things Are Considered in orthodonture and TMJ care
Click the plus sign below to read more information on each aspect of All Things Considered
The temporomandibular joint is one of the most frequently used and complex joints in the body. These joints are responsible for connecting the lower jaw to the skull. The TMJ is somewhat suspended in “space” by several ligaments and held in position by a ligamentous joint capsule. A certain amount of muscle and ligamentous tonicity is necessary to maintain a close, but translating connection to the skull.
A fibrous, but somewhat cartilaginous disc is normally positioned between the condylar head and skull to “protect” the cartilaginous articular surfaces. The position and controlled movement of the discs are controlled by ligamentous integrity and normal muscle contraction and relaxation.
The retrodiscal tissue (the tissue behind the condyle) is vascular and highly innervated, which makes this area exceptionally sensitive to inflammation and compression. The presence of a malocclusion can cause a TMJ dislocation, which typically will lead to joint noises, headaches and neck pain, and limited opening as well as osteoarthritis of the TMJ.

Of great importance in the orthodontic assessment is the relationship of the of the upper and lower jaws to each other and to the skull itself. You may find it interesting that all of the bones listed in the diagram to the left move to varying degrees; even the cranial bones. Added to this is the relationship that the cervical spine or neck has to the teeth and jaws. We are all aware that the lower jaw moves as does the cervical spine. However, as pointed out in osteopathic medicine, all of the cranial bones move to some degree as part of the cranial respiratory mechanism, which is the pumping mechanism that circulates the cerebral spinal fluid. The bones of the upper jaw or maxilla articulate via cranial sutures. The movement is slight but critical and measurable.
The mandible has two articulations with the temporal bone, one on each side. This articulation is called the temporomandibular joint. This joint is not a hinge joint but is suspended in space and is held in place by a fibrous capsule and fibrous ligaments.
The cervical spine is then connected to the skull with an articulation illustrated below:

As you gaze at the image to the left, you will notice the close relationship of the TMJ to the neck. What may be surprising is that all of these bones move at varying degrees. A fact that is seldom discussed or appreciated is the following:
If one has a malocclusion, it will adversely affect the TMJ as well as the cervical spine leading to dislocation. This misalignment of parts will lead to abnormal function eventually and significantly alter one’s posture over time. All of these parts are connected by muscles, tendons and fascia. In fact, the fascia connects all body parts via a web of connective tissue. In a very important sense, it connects all structures in the body.
In this picture, you can see a few of the cranial bones, the upper part of the cervical spine, the lower jaw (mandible), the TMJ, and the upper and lower jaws with teeth. Believe or not, all of these structures are moving parts held in suspension by muscles and ligaments.
If any of these bones are out of alignment, the body will compensate posturally; pretty much according to FORM and FUNCTION. If there is a dento-skeletal discrepancy creating a malocclusion, the body will adjust and compensate, but not without ultimately causing issues such as dislocation of the jaw joints and alteration of the cervical spine. Keep in mind, the muscles maintain a high level of tonus to allow us to function; however, this constant effort to maintain balance will eventually lead to alteration of posture, muscle spasm and referred pain.
So why is this important in the orthodontic world?
The challenge then is for the orthodontist to determine the degree of skeletal and dental imbalance and to identify any of the following below:
Most orthodontic problems are problems of bony deficiencies that determine the limits of dental positions. There are three planes of space that must be assessed: transverse, horizontal and vertical.
Transverse: is the jaw structure too narrow? Crowding or protrusion of the teeth is usually a problem of transverse deficiency; i.e. the upper and/or lower jaws are too narrow. For the best outcomes in medicine and dentistry, determine cause. In orthodontics, if narrow jaw structure exists, it is preferable to expand the dental arches in order to maintain all of the teeth. This is best done in a growing child, but can still be done in the adult patient.
Horizontal – The question is this: what is the relationship between the upper jaw and the skull followed by what is the relationship of the lower jaw to the upper jaw? Is it a growth and development problem or an orthopedic displacement? How are the teeth positioned within the confines of the jaw position: are the teeth protruded or too far forward, or retruded and too far back? And what influence do the teeth have on determining the position of the lower jaw? Is the lower jaw overdeveloped?
Vertical – is the lower face too long or too short? Did the upper jaw grow excessively in a vertical direction or not enough leading to a short lower facial height and “overclosure”?
Vertical – is the lower face too long or too short? Did the upper jaw grow excessively in a vertical direction or not enough leading to a short lower facial height and “overclosure”?
The basic but minimal standard of care requires two images: The lateral cephalogram and panorex


The next part of the diagnostic discipline is to objectively determine the relationship of parts as seen in the diagnostic illustrations below:

A receded lower jaw

Lower jaw asymmetry

Upper jaw deficiency or lower jaw excess

By outlining or tracing the various boney landmarks, the specialist is able to look at the dento-skeletal relationships more objectively, which in turn will point to a set of objectives that will be specific to the patient’s individual needs. Following this disciplined exercise an individualized treatment plan can then be formulated specific to the needs of the individual patient.
To answer the questions regarding the “planes of space” accurately will determine the specific treatment plan uniquely applied to each patient. Analysis, as illustrated above, is essential for each individual patient and determines the plan of orthodontic treatment . The orthodontist should be disciplined enough to assess the “parts” involved for a complete assessment for a definitive plan.
Another important image is the TMJ tomogram. The question to ask here is the following: is the lower jaw “receded” due to underdevelopment of the lower jaw or to orthopedic displacement of the lower jaw? In our opinion, an accurate diagnostic assessment cannot be achieved without imaging the TMJ.
Diagnostic Tomograms for the TMJ:

Condylar head dislocation (black arrows) and associated reduced joint space (red arrows). Due to the presence of a deep overbite, a narrow maxilla, and/or dental retrusion there will be a strong predisposition to mandibular “entrapment” resulting in dislocation of one or both of the jaw joints


An orthodontic assessment cannot be adequately done without considering the relationships of the upper jaw, lower jaw, cervical spine, the positions of the teeth within each jaw, and TMJ alignments to each other. Bones move and their respective functional alignments of one to another is critical.
Neuromuscular dentistry: Neuromuscular orthodontics and TMJ treatment differs from “traditional” orthodontics in the emphasis that is placed upon the activity of the muscles that move the jaw. Neuromuscular orthodontics positions the teeth and jaws in such a way as to maintain balance between the jaws, TMJ, teeth, and muscles. It recognizes that the muscles that move the jaw must be in a comfortable, relaxed position in order to not be in conflict with the teeth and the jaw joint. In another consideration, it emphasizes the position of the upper jaw as the template to which the lower jaw and the teeth must fit. Saying it another way, rather than violate the position and shape of the upper jaw, the position and shape of the upper jaw is either enhanced or at least not violated.


Background and Principles
It will be helpful to understand that the TMJ is considered to be the most unique and complicated of all joints in the body. It is actually “floating” in space. And it is the joint space that must be protected.
- All functional movements of the lower jaw begin and end in the rest position, which is entirely dependent upon the musculature.
- In its attempt to maintain balance or homeostasis, the mandible will always strive for a position of maximum stability. Because of the proprioceptive sensitivity of the mandible, a malocclusion can have devastating consequences to postural maintenance of the spine leading to chronic muscle hyperactivity and pain. Jankelson p. 12
- “While six pairs of muscles “control” chewing at least 40 pairs of muscles and ligaments will be affected by what is called the rest position of the lower jaw.” The Dental Physician, p. 96
- In fact, there are 16 sets of muscles that control the precise and sensitive movements of the lower jaw.
- These muscles and ligaments never rest but remain in a constant state of tonus or in state of partial contraction of some of its fibers.
- We must recognize that the skeletal bones are held together and positioned by muscles and ligaments. When one area is out of balance the remaining musculature and skeleton automatically assumes a balancing distortion due to this neuromuscular compensation.
- HOWEVER, if there is a malocclusion, then the neuromuscular physiology is disturbed and the patient will possess a pathologic and unstable rest position eventually leading to distress.
- When one area is out of balance the remaining musculature and skeleton automatically compensate leading to a balancing distortion.
Summary: A malocclusion is in a state of equilibrium; albeit a harmful state that will eventually lead to problems. If an orthodontist corrects the malocclusion without seeing to it that normal muscle activity is restored, optimal cervical spine alignment is achieved, and normal respiratory function is either maintained or corrected, then a state of disequilibrium will be the outcome leading to relapse and pain because the body wants balance.
- Proper stability of skeletal structures as well as synergistic function depend on the tonus of the musculature and ligaments.
- If correct rest position of the lower jaw exists, then and the skeletal supporting tonus and physiologic resting length of the musculature coincide.
- These muscles will then be in a state of improper tonus, and thus constitute a constant source of distress.
- It is important to recognize that the skeletal bones are held together and positioned by muscles and ligaments.
- A malocclusion or bad bite will usually cause dislocation of the TM joint and compromise the sensitive joint space. Unfortunately most orthodontic care provided today does not even consider the musculature or joint space for that matter. It is essential to do so to provide ultimate stability as a means of not causing other problems of postural compromise and neuromuscular dysfunction leading to compensating adjustments in posture and ultimately referred pain.
- Naso-respiratory distress often leads to postural compromise and neuromuscular dysfunction.
- The resting position of the lower jaw is established early in life even before the teeth have erupted.
- To emphasize these points another way, I will try the following scenario: A malocclusion is in a state of equilibrium; albeit a harmful state that will eventually lead to problems. If an orthodontist corrects the malocclusion without seeing to it that normal muscle activity is restored, optimal cervical spine alignment is achieved, and normal respiratory function is either maintained or corrected, then a state of disequilibrium will eventually be the outcome leading to relapse because the body wants balance.
According to Janet Travell, MD: Emeritis professor at George Washington University and White House physician under John F. Kennedy.
- Skeletal muscles (these are called the voluntary muscles) comprise the largest single organ in the body making up 40% or more of body weight.
- Yet these muscles receive little attention in the curricula in medical school teaching and medical textbooks.
- According Travell, these muscles are a major cause of pain and dysfunction in the largest organ of the body.
- These contractile muscle tissues are exceptionally subject to the wear and tear of routine activities, but providers spend more time looking at bones, joints, bursae and nerves than on abnormal muscle physiology and the concepts of referred pain.
- The tender areas in muscle are called trigger points. The muscular trigger point (TP) begins with muscular strain and quickly becomes the site of sensitized nerves, increased metabolism and reduced circulation.
- The TPs represent areas of ischemia or reduced blood flow, which means it is also an area of reduced oxygen.
- TPs are extremely common and become a distressing part of nearly everyone’s life from time to time.
- Latent TPs are far less common than active TPs and may cause stiffness and restricted range of motion.
- The TPs represent areas of ischemia or reduced blood flow, which means it is also an area of reduced oxygen.
- Skeletal muscles can become strained upon a sudden contraction or movement as well as repeated contraction due to the need to achieve balance between one body part to another.
- In other words, if there is a minor or major skeletal imbalance the muscles will compensate to maintain “balance” or structural homeostasis. This function usually requires repeated contractions and over time will lead to strain, muscle spasm and referred pain.
- Let’s just start with the illustrations below: All of the muscles in the head, neck and shoulder areas are under a constant state of contraction to help maintain head posture and a normal gaze upon the horizon.
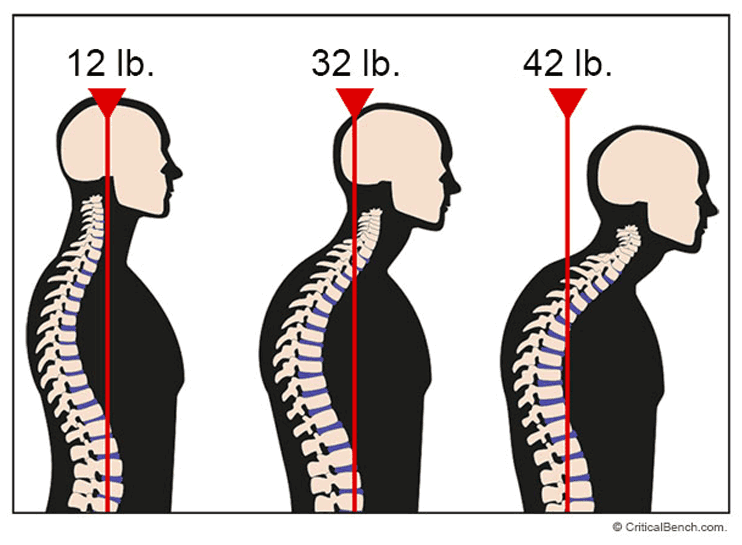
- In the presence of a malocclusion, the bones of the neck or cervical spine eventually come out of alignment. As in the “mouthbreather”, a forward head posture eventually occurs placing additional strain on the muscles of postural maintenance.
- As compensation is required, the forward head posture will be more noticeable over time placing more strain on these muscles. Eventually areas of reduced circulation will occur causing muscular hypoxia, which will in turn lead to acute and chronic headaches including migraines.
Abnormal Muscle Function and Referred Pain
Referred pain is pain felt at a site remote from the cause. Specifically, referred pain is pain that arises in a trigger-point, but is felt at a distance, often entirely remote from its source. These points are typically ischemic with reduced blood flow or reduced oxygenation usually associated with structural or postural imbalances and/or hypothyroidism (peripheral hypothyroidism). Common referred pain patterns that result from structural imbalances as seen in malocclusions and TMJ dislocation are illustrated below:
Other common areas of referred pain associated with common symptoms of jaw dysfunction:


The images illustrates trigger points in the sternocleidomastoid muscle (SCM). This is an important muscle of postural maintenance and can cause frontal headaches, pain behind the ear, and pain around eyes. In either case, the formation of trigger points can be related to hypo-metabolism (hypothyroidism) as described by Travell.

Spasms of the deep master muscle often refers pain to the ear causing one to think they have an ear infection. This part of the muscle can get activated or strained due to clenching or dislocation of the jaw joints.

The superficial master muscle can cause facial pain and jaw pain, as well as dental pain.


As stated earlier, spasm of the lateral pterygold muscle can refer pain to the cheek area or just in front of the ear on the affected side.
In other words:
- We want relaxed muscles to dictate jaw position to enhance long-term stability.
- That is, we want a muscle-dictated position rather than a doctor-dictated position.
- “Mouth breathing” can lead to abnormal head posture, which in turn can lead to muscle spasm within the jaw joint (lateral pterygoid muscle) as well as the masseter muscle. See the illustrations above:
- Poor circulation through a muscle can disrupt normal muscle activity or normal muscle physiology.
- Most of us have experienced a painful “Charlie horse” making it most difficult to even move a limb.
- This painful area is referred to as a myofascial trigger point (TP) within a taut band of skeletal muscle.
- This area or spot is painful upon compression and can refer pain to another area rather remote from the hyperirritable locus within the fascia or muscle itself.
- With reduced circulation you have reduced oxygenation causing the muscle to “cramp” or spasm.
- According to Travell, an active TP causes pain.
Another TP is called a latent TP, which is clinically silent with respect pain, but may restrict movement or cause muscle weakness. - Both active and latent TPs cause dysfunction; only active TPs cause pain. P.13
- Active TPs are most likely found in muscles of postural maintenance. These include postural muscles of the neck, masticatory, shoulder and pelvic muscles and are probably the most common cause of head and neck pain including headaches of the migraine-like intensity.
- Quite often, TMD causes a discoordination of the head, neck and jaw muscles causing pain or restricted movement.
- In the presence of a malocclusion, one’s posture will be compromised due to the compensatory nature of the body to establish and maintain equilibrium. A malocclusion will cause subluxation beginning with C1 and C2 over time eventually resulting in abnormal spinal alignment.
- Prolonged attempts to achieve homeostasis or balance when there is a persistent structural imbalance will lead to muscle spasm and morphologic changes over time.
- To emphasize these points another way, I will try the following scenario: A malocclusion is in a state of equilibrium; albeit a harmful state that will eventually lead to problems. If an orthodontist corrects the malocclusion without seeing to it that normal muscle activity is restored, optimal cervical spine alignment is achieved, and normal respiratory function is either maintained or corrected, then a state of disequilibrium will be the outcome leading to relapse because the body wants balance.
- One also has to consider the nutritional and systemic status to help develop and maintain equilibrium as well. For example, if one has too much calcium in their system, muscle spasm can result leading to referred pain. You see, calcium leads to muscle contraction whereas, magnesium is a muscle relaxant. Why? Too much calcium will suppress magnesium.
And around and around we go.
Traditional orthodontics can violate the upper jaw position through the use of headgear, extractions, or by simply not addressing an underdeveloped or malpositioned upper jaw, which in turn can violate the functional and structural integrity of the jaw joints. Neuromuscular orthodontics develops the upper jaw to its most optimal position and shape, then determines the most optimal lower jaw position where the muscles are relaxed and at rest. This is a three dimensional position in space and is often irrespective to the position of the teeth. We also factor in the jaw joint anatomy in determining the best lower jaw position for long-term stability. Our colleagues often refer to our practice as a TMJ-centered, airway centric orthodontic practice, which it is. When muscles are not in a relaxed state muscle spasm is often found. It is this area of spasm (trigger point) that can refer pain to areas remote from the source.
A poor bite or malocclusion eventually leads to a forward head posture ultimately violating the alignment of the spine beginning with subluxation of C1 and C2 as well as leading to dislocation of the jaw joints. In a book entitled The Dental Physician published in 1977, it was stated that one cannot correct the spinal alignment with any stability in the presence of a malocclusion of a bad bite. The poor posture then contributes to breathing difficulties, sleep problems, and further compensation in spinal alignment. Poor posture than places significant strain on the muscle of postural maintenance leading to referred pain.
Systemic Factors
The orthodontist must differentiate between the growing child and the adult patient when providing orthodontic care. Treating all ages the same can create some surprises along the way.
Airway considerations are a must in all ages. Failure to diagnose and manage airway obstruction will create instability in the final outcome.
Autoimmune issues need to be considered, ruled out or managed. Osteopenia and osteoporosis are also considerations. Methylation defects, vitamin B12 and folic acid deficiencies must be considered as well. Hormonal imbalances will differ from one patient to then next and change with age. All of these variables mentioned can affect the orthodontic process as well as the outcome.
The knowledgeable orthodontist is in a unique position to influence responsible lifestyle changes to insure the best possible outcome because of the commitment all parties have in a process that takes several months. This holds true regardless of the patient’s age.
If a patient has airway issues or allergies, the next question should be: Why is the body responding in this manner? One must always consider the “why” or the contributing factors behind the malocclusion in order to address cause. If a patient has a narrow palate, why did that happen? A narrow palate can be a sign of an abnormal tongue position caused by airway compromise [see Airway]. It also can be a sign of a previous or existing thumb habit.
Well, why is this important? Narrow jaw structure is typically the reason teeth protrude or crowd. Optimal tongue position influences normal development of the palate.
Hormonal Imbalances:
Low body temperature is often related to low thyroid function, which is an important player in normal muscle physiology. The thyroid hormone determines bone turnover rates, which is the basic biology of orthodontic tooth movement and bone remodeling.
Thyroid considerations apply to the TMJ/chronic pain patient as well as to the orthodontic patient. Low adrenal function can disrupt normal thyroid function. Adrenal function should be assessed prior to thyroid supplementation particularly in patients suffering from chronic pain and fatigue. Low thyroid can contribute to chronic sinus issues including allergies, which certainly should be considered in “mouthbreathers” as well as those suffering from sleep apnea. Low thyroid function has been implicated in childhood and adult ADHD. Low thyroid function is often due to iodine deficiency as well.
The bottom line: normal thyroid function determines normal bone turnover rates, the basic biology of tooth movement as well as normal muscle physiology. Since muscle spasm often refers pain to areas of the body remote from the spasm, normal thyroid function must be considered to bring balance to one’s physiology. Normal hormonal balance between production and secretion is dependent upon nutritional adequacy and balance beginning with mineral balance, which establishes the foundation for vitamins and enzymes to work within the body [see Nutrition].
Osteoporosis is another common diagnosis in the adult patient. Well, what about bone density for optimal periodontal health and the entire integrity of the skeletal system?
Let’s begin with the following scientific equation: Lysine + Proline + Vitamin C = Collagen
This equation simplifies a process needed to help insure bone density. It is a huge mistake to take calcium supplementation to help prevent osteoporosis; however, this recommendation is made quite commonly by physicians once women reach the age of 40. Not only is there insufficient scientific evidence to support this practice, this practice can be harmful as it will create mineral imbalances throughout the entire body.
Bone is comprised of about 12 different minerals plus a connective tissue matrix (collagen) into which the minerals deposit. In other words, collagen provides the infrastructure for mineral deposition leading to adequate bone density. To make matters worse, big pharma has come up with drugs to allegedly provide a remedy for osteoporosis or osteopenia.
This is a big problem as these drugs can interfere with bone remodeling and cause brittleness of the bones leading to death (necrosis) of the bone itself. Healthy bone has a degree of flexibility and should be allowed to respond to forces. Here we circle back to form and function.
Other problems are associated with excess calcium. In general, excessive amounts of any one mineral can suppress other minerals. We want mineral synergism not antagonism. Dr. Thompson in his book, Calcium Lie II, illustrates the sequence of events caused by excessive calcium. He calls this the Calcium Cascade and explains how this can contribute to hypothyroidism.
So why are we concerned about all of this? When helping patients eliminate headaches, I suggest that they discontinue the use of calcium supplementation or calcium rich foods. You see, calcium is a muscle contractor leading to muscle spasm, which is most often associated with referred pain. Don’t get me wrong. I am not even remotely suggesting that calcium is not important. I am suggesting that there is a good possibility that a mineral imbalance has been created over time leading to abnormal muscle physiology and questionable bone density. Rather than prescribe a muscle relaxant, I suggest magnesium supplementation as most everyone on the planet does not have enough of it.
Magnesium is a natural muscle relaxant, vasodilator, and equally or most importantly helps control blood viscosity. You see, we want our blood flowing like wine not like ketchup, which is somewhat of a mantra that we tell most of our patients dealing with systemic imbalances. Magnesium is also associated with over 800 different enzyme pathways throughout the body.
Are there side effects with magnesium? When first starting to use magnesium, it may have somewhat of a laxative effect depending on the type of magnesium that is used. I usually recommend magnesium glycinate as patients seem to do well with it.
However, there are other forms which are best purchased from a health food store. The big box stores have magnesium that is not well-absorbed or tolerated. Magnesium is the only mineral that I will recommend before specifically testing for mineral imbalances. Why? Most of us are deficient in magnesium as most of our farmland no longer has adequate levels of this mineral. Rather, mineral imbalances are currently the norm today.
How do we test for this to make sure that we are not creating other imbalances just through supplementation? Most of us might just suggest we obtain a blood test; however, 99% of our minerals are in our cells, not the blood stream.
Perhaps a tissue biopsy would provide more information. If you guessed that approach, you would be correct. That is why untreated hair is used as biopsy material. As crazy as it sounds, this is a method that has been used by medical laboratories for over 30 years. In fact, Dr. Thompson suggests that any doctor who is not doing a hair mineral analysis might just be bordering on malpractice. I am sure a strong comment like that just might endear him to the American Medical Association.
Here is the point: establishing mineral balance is foundational. We would not think of building a dream home without establishing a strong foundation. Then why do we treat our bodies with considerably less consideration?
Not too long ago, I was in Nevada completing my advanced certification in the use of medical ozone. I was demonstrating to a physician the intra-oral approach to using ozone for sinus infections and congestion. Upon finding out that he lives in Alaska, I asked him if he knew Dr. Thompson upon which he replied. “Yes I do. The guy
is brilliant!” You see, advances in medicine are only achieved when an individual has the compassion and courage “to step outside of the sacred box” called the Standard of Care. Most of us think that the term means excellence. Well not necessarily. The Standard of Care just means what everyone else is doing. We have come to understand that treating symptoms is just that: “Make my pain go away as fast as you can doctor.”
You see, failure to address the problem will ultimately result in failure. Years ago I questioned the lack of stability and the facial profile of many orthodontic patients; the standard of care was to remove teeth and/or use headgears. The specialty perhaps was not aware that the process would create problems years later.
In orthodontics, narrow jaw structure is the most common deficiency causing crowding and protrusion of the front teeth. The upper jaw is most often in a normal position from front to back, yet the use of headgear or extractions of teeth will violate the existing normal position leading to structural compensation and ultimately abnormal function: called the form / function relationship. In fact, this is a violation of oral volume predisposing one ultimately to sleep disordered breathing.
Airway is always a concern whether in a growing child or fully developed adult. A compromised airway will lead to abnormal facial development, narrow jaw structure, forward head posture, ADD and ADHD, cardiovascular compromise, diabetes, dementia and potentially Alzhiemer’s disease. Quite often patients will report having allergies, which in turn compromises airway leading again to compensation. Perhaps a better question should be this: “Why is your body responding in this manner?”
During my residency at the University of Michigan, we were required to do independent research suitable for publication to complete our master’s degree. My interest was in determining how we can improve long-term stability in the orthodontic outcome by establishing better bone density. I wanted to look at the relationship of vitamin C, magnesium and zinc to this end. I was told by my thesis chairman and the head of the Center for Human Growth and Development that I had too many variables, so just pick one. I chose vitamin C. This choice then mandated an animal study, one of which was never done previously.
As humans, we somehow lost the gene that tells our body to make its own vitamin C. The animal of choice was the guinea pig as it could not make its own vitamin C either. Well, how would this test the orthodontic question? Yes, I did put braces on several guinea pigs, but not all of them. You see, we needed controls meaning untreated animals that received vitamin C supplementation as well. Some tooth movement would be required to test the boney remodeling and quality of bone turnover rates with various quantities of vitamin C administered on a daily basis.
My hypothesis was this: could better bone density and/or quality of bone provide improved orthodontic outcomes in the area of long-term stability? So we set sails to evaluate bone density.
Bear with me here as this can get a little complicated. We had two groups: treated and untreated. Within each of these groups we had three subgroups with the only differentiation being the amount of vitamin C administered on a daily basis. We supplemented vitamin C using the following guidelines: dosing the recommended daily allowance, 10x more than the recommended allowance, and 10x less (deficient) then the recommended allowance. In the recommended allowance and deficient groups we observed very poor connective tissue or collagenous matrix resulting in poor bone quality. In fact, there were actual voids in the bone. In the 10x groups we observed what I have often referred to has an artist’s rendering of collagen and bone quality with absolutely no voids.
My thesis chairmen, a well-published anthropologist, Dr. Melvin Baer, was astonished and called Dr. Enlow the world’s expert on growth and development and asked him if rodents have Haversian systems as humans do. He stated that he had never seen them in rodents and that such a structural advancement does not exist in rodents. Dr. Baer to Enlow, well we are looking at them under the microscope. The point of all of this is the difference an adjustment in one variable can make.
Fast forward a few years, a German physician, Dr. Mathias Rath developed a nutritional supplement comprised of lysine, proline, and vitamin C while stating that one cannot get metastatic cancer if one has dense connective tissue. My point is this: nutrition is critical and guided supplementation is often needed unless you are growing your own food on mineral rich soils if you desire to enjoy optimal health.
Unfortunately, Western medicine as we know it can best be described as the following: “a drug for a bug (symptom); call me the next time you are sick.” Rather easy when compared to taking the time and effort to determine why one’s body is responding to an event, imbalance, or negative thought the way it does. I call this “peeling the onion one layer at a time.”
Nutrition: Deficiencies and Excesses
Poor nutrition often leads to poor dental and facial skeletal development as pointed out by Dr. Westin Price in the 1930’s. “Mouthbreathing” is often related to poor nutrition because of swollen lymphoid tissue causing obstruction to normal nasal breathing leading to abnormalities in dento-skeletal development, postural compromise, as well as attention deficit in children and adults.
Nutritional adequacy is critical for normal growth and development as well as for maintenance and repair. Our bodies use countless mechanisms, strategically placed throughout our digestion, absorption, and transport and metabolic pathways, to effortlessly ensure tissue concentrations consistent with good health. In short, your body is constantly monitoring and adjusting the concentrations of nutrients in the food you consume to turn massive variability into the narrower ranges required to establish and maintain health.
Mineral Imbalances:
Mineral imbalances can lead to muscle spasm and referred pain. For example, excess calcium can lead to over-contraction of muscles resulting in referred pain; meaning the pain is experienced in an area remote from the problem. Imbalances can also disrupt adrenal function, which in turn can block the normal conversion of T4 (inactive thyroid hormone) to T3 (active thyroid hormone) contributing to hypothyroidism. The active thyroid hormone T3 is responsible for proper conversion of fats to energy within the mitochondria.
Excess calcium can also suppress potassium. Potassium is critically important for a normally functioning thyroid. Calcium can be antagonistic to magnesium, a mineral that is critically important for normal muscle physiology, heart function, and energy production within our mitochondria as well. Balance is achieved when these minerals have a synergistic relationship rather than an antagonistic one. You see, too much of one mineral can suppress another.
To make matters a little more challenging is the fact that minerals must work together. Too much of one may suppress another. Mineral relationships must be synergistic, not antagonistic.

The mineral wheel diagrammatically indicates the mineral relationships and the balance that must be established to maintain health. Too much of one mineral will tend to suppress another. As we can see, an elevated mineral can effect two or more minerals.
The problems of deficiencies starts with the nutrient balance in our soils.

Our nutrition is only as good as the nutrients that are actually in our soil.
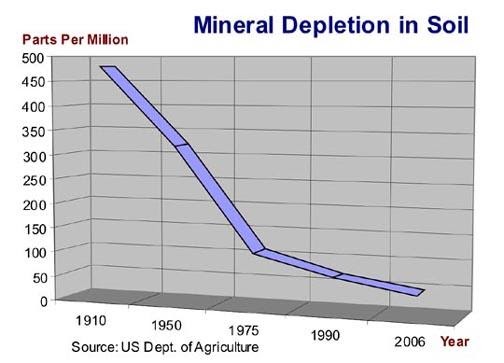
There are two classes of minerals, MAJOR and TRACE. Even though trace minerals are required in very small amounts, they are indeed essential to good health.
What about bone density for optimal periodontal health and the entire integrity of the skeletal system?
Let’s begin with the following scientific equation: Lysine + Proline + Vitamin C = Collagen
This equation simplifies a process needed to help insure bone density. It is a huge mistake to take calcium supplementation to help prevent osteoporosis; however, this recommendation is made quite commonly by physicians once women reach the age of 40. Not only is there insufficient scientific evidence to support this practice, this practice can be harmful as it will create mineral imbalances throughout the entire body. Bone is comprised of about 12 different minerals plus a connective tissue matrix (collagen) into which the minerals deposit.
In other words, collagen provides the infrastructure for mineral deposition leading to adequate bone density. To make matters worse, big pharma has come up with drugs to allegedly provide a remedy for osteoporosis or osteopenia. This is a big problem as these drugs can interfere with bone remodeling and cause brittleness of the bones leading to death (necrosis) of the bone itself. Healthy bone has a degree of flexibility and should be allowed to respond to forces. Here we circle back to form and function.
Other problems are associated with excess calcium. In general, excessive amounts of any one mineral can suppress other minerals. We want mineral synergism not antagonism. Dr. Thompson in his book, Calcium Lie II, illustrates the sequence of events caused by excessive calcium. He calls this the Calcium Cascade and explains how this can contribute to hypothyroidism.
So why are we concerned about all of this? When helping patients eliminate headaches, I suggest that they discontinue the use of calcium supplementation or calcium rich foods. You see, calcium is a muscle contractor leading to muscle spasm, which is most often associated with referred pain. Don’t get me wrong. I am not even remotely suggesting that calcium is not important. I am suggesting that there is a good possibility that a mineral imbalance has been created over time leading to abnormal muscle physiology and questionable bone density. Rather than prescribe a muscle relaxant, I suggest magnesium supplementation as most everyone on the planet does not have enough of it.
Magnesium is a natural muscle relaxant, vasodilator, and equally or most importantly helps control blood viscosity. You see, we want our blood flowing like wine not like ketchup, which is somewhat of a mantra that we tell most of our patients dealing with systemic imbalances. Magnesium is also associated with over 800 different enzyme pathways throughout the body.
Are there side effects with magnesium? When first starting to use magnesium, it may have somewhat of a laxative effect depending on the type of magnesium that is used. I usually recommend magnesium glycinate as patients seem to do well with it. However, there are other forms which are best purchased from a health food store. The big box stores have magnesium that is not well-absorbed or tolerated. Magnesium is the only mineral that I will recommend before specifically testing for mineral imbalances. Why? Most of us are deficient in magnesium as most of our farmland no longer has adequate levels of this mineral. Rather, mineral imbalances are currently the norm today.
How do we test for this to make sure that we are not creating other imbalances just through supplementation? Most of us might just suggest we obtain a blood test; however, 99% of our minerals are in our cells, not the blood stream. Perhaps a tissue biopsy would provide more information. If you guessed that approach, you would be correct. That is why untreated hair is used as biopsy material. As crazy as it sounds, this is a method that has been used by medical laboratories for over 30 years. In fact, Dr. Thompson suggests that any doctor who is not doing a hair mineral analysis might just be bordering on malpractice. I am sure a strong comment like that just might endear him to the American Medical Association.
Here is the point: establishing mineral balance is foundational. We would not think of building a dream home without establishing a strong foundation. Then why do we treat our bodies with considerably less consideration?
Not too long ago, I was in Nevada completing my advanced certification in the use of medical ozone. I was demonstrating to a physician the intra-oral approach to using ozone for sinus infections and congestion. Upon finding out that he lives in Alaska, I asked him if he knew Dr. Thompson upon which he replied. “Yes I do. The guy
is brilliant!” You see, advances in medicine are only achieved when an individual has the compassion and courage “to step outside of the sacred box” called the Standard of Care. Most of us think that the term means excellence. Well not necessarily. The Standard of Care just means what everyone else is doing. We have come to understand that treating symptoms is just that: “Make my pain go away as fast as you can doctor.”
You see, failure to address the underlying problems will ultimately result in failure. Years ago I questioned the lack of stability and the facial profile of many orthodontic patients; the standard of care was to remove teeth and/or use headgears. The specialty perhaps was not aware that the process would create problems years later.
In orthodontics, narrow jaw structure is the most common deficiency causing crowding and protrusion of the front teeth. The upper jaw is most often in a normal position from front to back, yet the use of headgear or extractions of teeth will violate the existing normal position leading to structural compensation and ultimately abnormal function: called the form / function relationship. In fact, this is a violation of oral volume predisposing one ultimately to sleep disordered breathing.
Airway is always a concern whether in a growing child or fully developed adult. A compromised airway will lead to abnormal facial development, narrow jaw structure, forward head posture, ADD and ADHD, cardiovascular compromise, diabetes, dementia and potentially Alzheimer’s disease. Quite often patients will report having allergies, which in turn compromises airway leading again to compensation. Perhaps a better question should be this: “Why is your body responding in this manner?”
During my residency at the University of Michigan, we were required to do independent research suitable for publication to complete our master’s degree. My interest was in determining how we can improve long-term stability in the orthodontic outcome by establishing better bone density. I wanted to look at the relationship of vitamin C, magnesium and zinc to this end. I was told by my thesis chairman and the head of the Center for Human Growth and Development that I had too many variables, so just pick one. I chose vitamin C. This choice then mandated an animal study, one of which was never done previously. As humans, we somehow lost the gene that tells our body to make its own vitamin C. The animal of choice was the guinea pig as it could not make its own vitamin C either. Well, how would this test the orthodontic question? Yes, I did put braces on several guinea pigs, but not all of them. You see, we needed controls meaning untreated animals that received vitamin C supplementation as well. Some tooth movement would be required to test the boney remodeling and quality of bone turnover rates with various quantities of vitamin C administered on a daily basis. My hypothesis was this: could better bone density and/or quality of bone provide improved orthodontic outcomes in the area of long-term stability? So we set sails to evaluate bone density.
Bear with me here as this can get a little complicated. We had two groups: treated and untreated. Within each of these groups we had three subgroups with the only differentiation being the amount of vitamin C administered on a daily basis. We supplemented vitamin C using the following guidelines: dosing the recommended daily allowance, 10x more than the recommended allowance, and 10x less (deficient) then the recommended allowance. In the recommended allowance and deficient groups we observed very poor connective tissue or collagenous matrix resulting in poor bone quality. In fact, there were actual voids in the bone. In the 10x groups we observed what I have often referred to has an artist’s rendering of collagen and bone quality with absolutely no voids.
My thesis chairmen, a well-published anthropologist, Dr. Melvin Baer, was astonished and called Dr. Enlow, the world’s expert on growth and development and asked him if rodents have Haversian systems as humans do. He stated that he had never seen them in rodents and that such a structural advancement does not exist in rodents. Dr. Baer to Enlow, “well we are looking at them under the microscope.” The point of all of this is the difference an adjustment in just one variable can make. Fast forward a few years, a German physician, Dr. Mathias Rath developed a nutritional supplement comprised of lysine, proline, and vitamin C while stating that one cannot get metastatic cancer if one has dense connective tissue. My point is this: nutrition is critical and guided supplementation is often needed unless you are growing your own food on mineral rich soils if you desire to enjoy optimal health.
Unfortunately, Western medicine as we know it can best be described as the following: “a drug for a bug (symptom); call me the next time you are sick.” Rather easy when compared to taking the time and effort to determine why one’s body is responding to an event, imbalance, or negative thought the way it does. I call this “peeling the onion one layer at a time.”
Vitamin D:
Deficiency of vitamin D is epidemic. It affects our entire immune system. A lack of vitamin D may play a role in chronic pain caused by a variety of conditions, though the exact link is not clearly defined. Research has indicated vitamin D deficiency may be implicated in musculoskeletal conditions, such as rheumatoid arthritis, neuropathy, migraine, inflammation as well as vertigo.
Vitamin D3 has been called a fat soluble vitamin for years. Interestingly enough, it is not a vitamin at all but a pro-hormone. It helps calcium absorption. However, one should not supplement with vitamin D3 without taking vitamin K2 with it. It is my understanding that K2 directs the absorbed calcium to be stored in the bone rather than letting it accumulate in our arteries, muscle and ligaments.
Researchers reported in the journal Neurology that low blood levels of vitamin D are also associated with a greater likelihood of developing Alzheimer's disease. The subjects did not have dementia at the beginning of the study. Volunteers with vitamin D levels of less than 25 nmol/L were twice as likely to have Alzheimer's disease or another dementia at a follow-up five years later.
Studies show that vitamin D regulates many functions in the body, including hormone balance, metabolism, blood pressure, bone density, fighting cancer, and immune function (ever notice that people tend to get colds and flu in the winter when the sun is low?). Vitamin D is critical for our health. We know that vitamin D is essential for healing and protecting against many contagious diseases and chronic diseases. Low levels of vitamin D are associated with upper and lower respiratory infections, heart disease, asthma, cancers, diabetes, multiple sclerosis, HIV, hypertension, inflammatory bowel disease, Alzheimer’s disease and other autoimmune diseases. Vitamin D deficiency is a worldwide public health problem in both developed and developing countries.
Vitamin D actually influences the expression of over 200 health-supporting genes in our bodies. There’s a lot of buzz about vitamin D boosting immune function to fight off colds, seasonal influenza, and other viruses. Research suggests that vitamin-D deficiency may one of the primary reasons people get more colds and flu in the winter when sunshine is less available.
Vitamin D works to strengthen this innate immune system response. Many different studies have associated vitamin D with its power to fight infection. One report looked at almost 19,000 people and found that the individuals with the lower levels of vitamin D were more likely to report upper respiratory tract infections, than those with sufficient levels of vitamin. It works by boosting the strength of the immune system while lowering inflammatory reactions. This makes vitamin D a powerful immune modulator. It helps boost immune power, but prevents the immune system from overreacting, as in the case of autoimmune disease.
So why are we messing with all of this anyway? I will list a few thoughts for consideration below:
- If poor nutrition often leads to poor dental and facial skeletal development according to Dr. Westin Price in the 1930’s, we would like to reverse this trend.
- The abnormal dento-skeletal development leads to a bad bite or malocclusion
- The poor bite leads to a forward head posture ultimately violating the alignment of the spine beginning with subluxation of C1 and C2 as well as leading to dislocation of the jaw joints.
- In a book entitled The Dental Physician published in 1977, it was stated that one cannot correct the spinal alignment with any stability in the presence of a malocclusion of a bad bite.
- The poor posture then contributes to breathing difficulties, sleep problems, and further compensation in spinal alignment
- Basically, vitamin D3 is critical to prevent pain, prevent or manage autoimmune disease, maintain normal respiratory function, and strengthen our immune system.
Is this diagnostic discipline widespread and a standard of care? Sadly, no it is not. Actually, orthodontics is considered the most demanding and difficult of all dental specialties that requires non-stop thinking and assessment initially and throughout the entire process. It takes time to properly assess the problem, care in developing an appropriate plan of care, and careful communication to enhance a functional understanding. It has often been said that dentistry is the largest medical specialty. In my opinion, orthodontics should be a medical specialty demanding more assessment and care than currently exists in the marketplace.
We are now seeing the implementation of the corporate structure in medicine and dentistry. As corporations go, the business model is one of production. Several years ago I got caught up in that management style so I could spend more time seeing patients and let others manage the business of healthcare; meaning corporate management. Several of my colleagues had made the decision to move in that direction, so I followed suit. It did not take me very long to realize that the doctor – patient relationship suffered along with the quality of care throughout the industry. The time the doctor had with each patient could be measured in seconds. A non-orthodontic specialist was achieving better results than the university trained specialist. Ah, the temptations in the market place are driven by the pressure to produce according to insurance mandates that says to the provider: “accept a lesser fee and make it up in volume.” This is impossible to do when one considers the need for a thorough diagnostic assessment and plan of care. We have learned that what an orthodontist does or does not do can affect a patient for the rest of their lives either positively or negatively.
So why are we messing with all of this anyway? I will list a few thoughts for consideration below:
- “Mouthbreathing” is often related to poor nutrition because of swollen lymphoid tissue causing obstruction to normal nasal breathing leading to abnormalities in dento-skeletal development, postural compromise, as well as attention deficit in children and adults.
- The abnormal dento-skeletal development leads to a bad bite or malocclusion.
- The poor bite leads to a forward head posture ultimately violating the alignment of the spine beginning with subluxation of C1 and C2 as well as leading to dislocation of the jaw joints.
- In a book entitled The Dental Physician published in 1977, it was stated that one cannot correct the spinal alignment with any stability in the presence of a malocclusion of a bad bite.
- The poor posture then contributes to breathing difficulties, sleep problems, and further compensation in spinal alignment



In between structural and systemic issues is the area of “mouthbreathing”. It can be considered structural in the sense that one may have obstruction to normal nasal airflow such as enlarged turbinates in the nose. It can be considered systemic as it has a lot to do with oxygenation and normal muscle physiology among other things. In fact, airway obstruction is now considered to be an important contributing factor to ADD, ADHD, and sleep disordered breathing and clenching.
“Mouthbreathing”, as opposed to nasal breathing, negatively influences facial growth and development in the growing child as well as postural maintenance of the head and neck areas in suboptimal positions, which can ultimately lead to alignment problems along the entire spine. Forward head posture typically occurs in “mouthbreathers” leading to muscle compensation and spasm. This forward head posture places considerable strain on the muscles of postural maintenance such as the trapezius muscles (shoulder muscles). Other muscles of postural maintenance are effected as well. Airway should be one of the first concerns of an orthodontist.
“Mouthbreathing” may be related to a nasal obstructions that typically show up on x-rays as enlarged adenoids, turbinates, nasal septal deviation, or enlarged tonsils. It is often related to soft tissue collapse deeper in the throat. As far as we know, we are the only office in the Atlanta area using reflective acoustic wave technology using sound waves to non-invasively measure any degree of obstruction in the nose as well as the degree of soft tissue “collapse” in the throat. We use this in growing patients as well as those suffering with sleep apnea or sleep disordered breathing. However, chronic sinus issues may be due to allergies with an underlying cause being related to vitamin D3 deficiency, low thyroxin (thyroid hormone), or a culinary lifestyle of high gluten-related foods and dairy.
THE TEETH
A malocclusion is a misalignment or incorrect relation between the teeth of the two dental arches when they approach each other as the jaws close. Poor relationships of the upper and lower teeth can contribute to dislocation of the jaw joint. Most people are concerned about how their teeth look. Seldom does anyone think about function and how the teeth can be related to spinal alignment and to cardiovascular disease.
The longer a malocclusion exists, increasing damage to the cervical spine (neck) is expected. Orthodontic correction accomplished without an awareness of TMJ integrity can cause dislocation of the TMJ as well leading to postural abnormalities and unfavorable compensations. In a sense, posture begins in the mouth.
Crowding of the teeth interferes with oral hygiene resulting in conditions leading to periodontal disease (bleeding gums), bone loss and decay. These conditions increase the likelihood of developing cardiovascular disease as well.
A malocclusion can be subtle or obvious. Examples of a malocclusion are illustrated below:
Deep Overbite

Narrow Jaw Structure

Dental retrusion (upper teeth pushed-back)



Openbite

Crowding





Why Choose Dr. Dierkes?
The only neuromuscular orthodontist in GA.
Advanced certification in the use of medical ozone for migraines, headaches, neck pain and chronic sinusitis.
He is the only orthodontist in Georgia conservatively treating the TMJ patient with Prolozone, and trigger point injections
The most advanced and safest imaging available
The most experienced orthodontist in early, interceptive treatment.
Takes a holistic approach to care.
Dr. Dierkes works on you and spends as much time with you as the clinical assistant does
Attention to detail in evaluating systemic factors influencing the quality of the final results.
Kind Words
Dr.Dierkes was my orthodontist from a child all the way to out of high school. He is the best and knowledge goes beyond just orthodontics. He’s friendly, helpful and wants the best for his clients. I now have a perfect smile that I can credit to him.
I have known this master of orthodontics for over 20 years He is a beacon in Roswell and he gave my daughter a million dollar smile . I am so greatful for his expertise and kindness. Thankyou Dr Dierkes
Dr Dierkes is an amazing orthodontist with a holistic approach to health. He advocates doctors working together to bring harmony to the body. I'm really impressed with his knowledge and care for medicine and for his patients. If you or anyone in your family are in need of braces, you should start looking for his opinion and then make your decision. You will chose with him for sure!

Schedule Your First Visit Today
JM Dierkes Orthodontics and TMJ is more than happy to submit all insurance forms for you to help you recover the most from your benefits. We will do everything we can to help you afford the treatment you need and want
Contact us today to schedule you or your child's first appointment with us.